Understanding, Diagnosis, and Treatment of Glaucoma
The development of the indentation tonometer had a major
impact on the definition of glaucoma. With a more quantitative and accurate
method of measuring intraocular pressure, the indentation tonometer had a
strong influence on the understanding, diagnosis, and treatment of glaucoma in
the early 1900s. At this time in the history of medicine, there was a strong
shift in the standardization and efficiency of medical care. In many fields of medicine, there were new
instruments and technologies being adopted into clinical practice. A 1918 American Journal of Ophthalmology
article by M. Uribe-Troncoso stressed the importance and benefits of the widespread
usage of tonometers in routine eye exams to monitor and make clear diagnoses of
glaucoma. For the first time, intraocular pressure could be recorded in a
quantitative manner and be monitored in a more precise, less subjective way.
Ophthalmologist began to depend more on intraocular pressure measurements to
access the eye health of their patients.
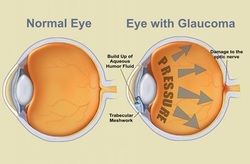 Image 7: A normal eye versus an eye with glaucoma
Image 7: A normal eye versus an eye with glaucoma
"A wider use of the tonometer is a necessity and will make clear the diagnosis in many obscure cases. It is to be hoped that such a good instrument will find its way into a more general use."
-M. Uribe-Troncoso, American Journal of Ophthalmology, 1918
-M. Uribe-Troncoso, American Journal of Ophthalmology, 1918
An increase in intraocular pressure was found to be one of the main risk factors for glaucoma. With this new method for measuring eye pressure, there had to be standards established as to what normal IOP readings were. This brought about much debate. Intraocular pressure is maintained by the proper outflow of aqueous humor, the fluid in the eye. An increase in pressure is the result or improper drainage of the aqueous humor and this build up in pressure can lead to damage of the optic nerve (image 7). Many manometry experiments were conducted on the eyes of dogs and rabbits to assess a reference intraocular pressure and then compare the readings from different types of tonometers. Manometry is an invasive technique that gives the direct measurement of eye pressure by inserting a needle into the eye. The indentation tonometers where calibrated according to the manometer intraocular pressure of cadaver eyes. For the Schiötz tonometer, 14 mmHg was considered to be the normal intraocular pressure. Although this was considered normal for the Schiötz tonometer, other instruments, like the McLean had different definitions of normal. This led to some confusion and inconsistencies in the measurement of eye pressure. The readings of the indentation tonometers also depended on other properties of the eye, including ocular rigidity, which is the stiffness or elasticity of the cornea. This varies from patient to patient and is higher for hyperopic eyes than myopic eyes. Therefore, for someone who is hyperopic, the indentation tonometer would be expected to overestimate the intraocular pressure. Schiötz acknowledged this issue in this report of the Schiötz tonometer in the British Journal of Ophthalmolgy by simply stating, “I can not imagine any method available for living eyes by which errors due to variations in the envelope could be eliminated” (1920).
Along with standardizing the human eye and shaping the medical understanding of glaucoma, the ability to measure pressure led to ophthalmologists’ dependence on the instrument to diagnosis and treat glaucoma. This had both positive and negative effects on ophthalmic care. Before the use of the tonometer, many doctors were not recognizing glaucoma until it was too advanced for treatment (Brown 1920). The tonometer allowed medical practitioners to better understand intraocular pressure and monitor their patients, but it also lead to a dependence on the quantitative parameter to define the disease. A Gaussian distribution of the population was assumed in order to define glaucoma as any eye pressure outside two standard deviations of the average. Diagnoses where made based solely on a high intraocular pressure reading; when the reading was over 21 millimeters of mercury, many practitioners considered the patient to have glaucoma (Stamper). It was faintly realized that there could be a high IOP without glaucoma or a normal IOP with glaucoma, but for the majority of cases, treatments (both medicinal and surgical) where used until the IOP was lowered. Some of the most common surgeries included iridectomies, in which part of the iris was removed and filtering operations. In the early 1900s, there was also the discovery of hypotensive drugs the eyes that lowered the pressure including pilocarpine and epinephrine (Kronfeld).
Along with standardizing the human eye and shaping the medical understanding of glaucoma, the ability to measure pressure led to ophthalmologists’ dependence on the instrument to diagnosis and treat glaucoma. This had both positive and negative effects on ophthalmic care. Before the use of the tonometer, many doctors were not recognizing glaucoma until it was too advanced for treatment (Brown 1920). The tonometer allowed medical practitioners to better understand intraocular pressure and monitor their patients, but it also lead to a dependence on the quantitative parameter to define the disease. A Gaussian distribution of the population was assumed in order to define glaucoma as any eye pressure outside two standard deviations of the average. Diagnoses where made based solely on a high intraocular pressure reading; when the reading was over 21 millimeters of mercury, many practitioners considered the patient to have glaucoma (Stamper). It was faintly realized that there could be a high IOP without glaucoma or a normal IOP with glaucoma, but for the majority of cases, treatments (both medicinal and surgical) where used until the IOP was lowered. Some of the most common surgeries included iridectomies, in which part of the iris was removed and filtering operations. In the early 1900s, there was also the discovery of hypotensive drugs the eyes that lowered the pressure including pilocarpine and epinephrine (Kronfeld).
It wasn’t until the mid-1960s that the true definition of glaucoma began to be questioned as more than just elevated intraocular pressure. Population studies in the Rhondda valley, Wales by Hollows and Graham showed the distribution of intraocular pressure and the prevalence of glaucoma of all types. The results for the distribution of intraocular pressure, as reported in the British Journal of Ophthalmology, are shown below (image 8). The article also stresses the importance of basing upper levels of normality of intraocular pressure on more than just tonometric statistics, including cupping of the optic disc and visual field loss. Hollows and Graham defined different types of glaucoma, including Low Tension Glaucoma, in which tonometry readings where not over 21 mmHg, but glaucoma was present.
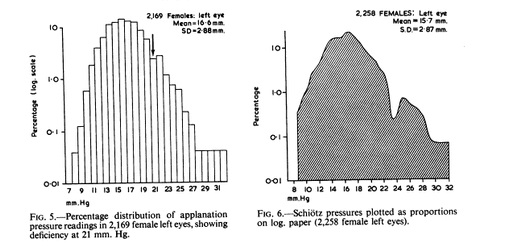
Image 8: Findings of the Wales population study. The results addressed the fact that the data does not have a true normal distribution, and therefore glaucoma diagnosis should not be based on standard deviation.
A pivotal point in the understanding between intraocular pressure and glaucoma came in 1962, when Mansour Armaly studied the correlation between pressure levels and the development of glaucoma in a Des Moines, Iowa population study. The findings of the study showed that there wasn’t the strong correlation between elevated intraocular pressure and development of glaucoma and visual field loss. Of those with a Schiötz reading over 21 mmHg, only a small percentage actually developed glaucoma and experienced visual field loss over a 7 year period (Armaly 1962). This study and many others of similar findings, showed tonometry readings could no longer be counted on for diagnostic purposes alone, but still played a role in the management of intraocular pressure.
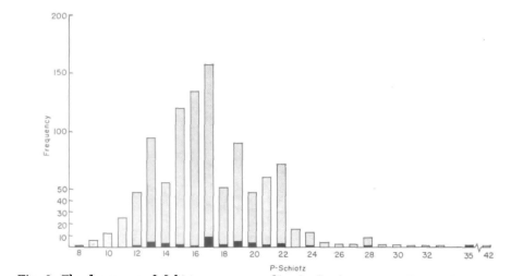
Image 9: The distribution of Schiotz pressure readings of patients at their first examination. The light bars are those with normal visual fields and the dark bars are those who showed visual field loss.
